Purpose
Observe from the hip joint to the knee joint, for diagnosis of dislocation, fractures, osteomyelitis, and foreign bodies.
Prior confirmation
For adults, the knee joint and hip joint should be projected along the diagonal of a 17×14 inch size. If they do not fit within this size, a judgment should be made whether to prioritize the hip joint or the knee joint for imaging, or to capture the images in two separate exposures.
Remove any obstacles.
Positioning




Supine oblique position with the affected side down.
Slightly flex the knee of the affected side (0-45°) and ensure the lateral aspect of the thigh is in contact with the table.
Align a line connecting the medial and lateral condyles of the femur perpendicular to the table.
The non-affected leg should be abducted, and the knee flexed.
Align the knee joint to the corner of the irradiation field.
Adjust the angle of the irradiation field so that the hip-joint projects to the opposite corner.
Place the cassette according to the irradiation field.
Cover any unnecessary irradiated area with a lead plate.
Place the R/L marker.
CR, distance, field size
CR : Perpendicular beam directed towards the center of the femur.
Distance : 100cm
Field size : Include the hip joint to the knee joint, encompassing the skin surface. It can also show lateral aspects by including the obturator foramen.
Exposure condition
70kV / 10mAs
Grid ( + )
Image, check-point
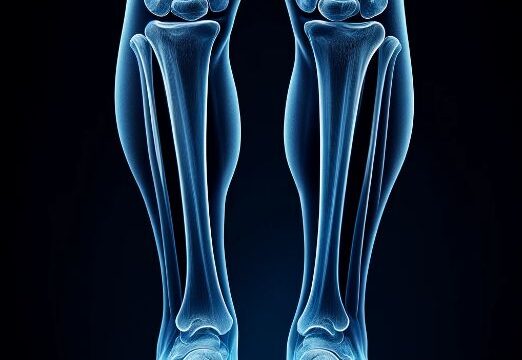
Normal (Radiopaedia)


The image should include the region from the hip joint to the knee joint.
The patella should be projected laterally, and the femoropatellar joint should be visible.
The head of the fibula (1/2 to 1/3) should overlap the tibia.
A portion of the lesser trochanter and the entire greater trochanter should be projected, overlapping the femoral shaft.
Cortical and medullary portions of the femoral shaft should be clearly observed.
The non-affected lower limb should not overlap.
There should be sufficient tolerance to observe soft tissue structures.
The RL marker should be present.
There should be no motion blur.
Videos
Related materials